Common responses to stress include eating more ice cream, watching more TV shows, and the more physiologically relevant development of clenching every muscle in your body. Today, stress is seen as a well-established accompaniment to muscle tension.
The relationship between stress and muscle tension is multifaceted. While both are interlinked, a hypothesis called the facial feedback mechanism goes so far as to say that muscle tension can exacerbate feelings of stress. The Facial Feedback Hypothesis, first introduced by Charles Darwin in 1872, essentially proposed that facial expressions, which are manifestations of muscle contractions, have a direct effect on mood. Some people claim that if you smile enough, you will start to feel happy.¹ The facial feedback hypothesis supports this thought and also suggests the reverse: if you frown, tense up, or employ any other bodily expression associated with negative emotions, those negative emotions will likely be reflected in one’s internal state or mood.¹ This suggests that the body has memories associated with certain muscle tensions. Because the body already associates stress-related muscle tension with negative affective states like stress and depression, continuing to tense our muscles even when we do not feel these negative emotions can send signals back to the brain, a development that can turn a positive mood negative.²
Researchers have opened new avenues to study the relationship between the facial feedback loop and depressive moods.³ Promising research in this area has potentially found a way to alleviate depression through an unorthodox method of reducing muscle contractions–Botox. This novel treatment method involves the administration of Botox, which is a compound more widely known for its role in cosmetics rather than for its salutary applications.
Before discussing specific research methods, it is important to understand the characteristics and mechanisms involved in muscle contraction. For us, voluntary muscle contractions seemingly occur without much thought; if you intend to move your arm, your arm moves. However, every conscious movement is actually the result of an intricate series of steps. More specifically, the interactions between neurons and muscle fibers actually help initiate muscle movement.
Neurons communicate with muscle fibers through chemicals called neurotransmitters. One such neurotransmitter is acetylcholine. Here, acetylcholine triggers a series of changes that result in an action potential, or the rapid change of charge, in a muscle fiber, and ultimately leads to muscle contraction.
Neuronal axon terminals contain vesicles that carry acetylcholine. Acetylcholine gets transported from the axon terminal to the presynaptic membrane, where it diffuses across the synaptic cleft and binds to receptors on the muscle fiber. Here, the presynaptic membrane refers to the portion of the axon terminal that faces the muscle fiber, and the synaptic cleft is the space between a neuron and a muscle fiber. To first bring the acetylcholine-containing membranes closer to the presynaptic membrane, synaptotagmin, a protein in the axon terminal, pinches the basement membrane of the terminal towards the oncoming vesicle. The basement membrane itself contains proteins called syntaxin and SNAP-25. On the vesicle membranes is a protein called synaptobrevin. The interaction between syntax-in, SNAP-25, and synaptobrevin creates a helical bundle, forming the SNARE complex. The SNARE complex brings the vesicles containing acetylcholine closer to the presynaptic membrane, allowing for fusion between vesicle and membrane and for the exocytosis of acetylcholine out of the synaptic terminal and towards the muscle fiber, where it can then bind to receptors and initiate a series of changes that trigger a muscle action potential and ultimately a muscle contraction.
Although muscle contractions serve an important function in voluntary physical movement, certain beauty products have moved to capitalize on muscle paralysis. At first glance, we may think that all paralysis is medically undesirable; after all, it takes away a muscle’s ability to contract, and a body’s ability to move.
A certain form of flaccid paralysis, however, represents an essential form of treatment in the cosmetic industry, and even young people are keen to undergo such treatments as preventative measures. To achieve results, many are using the botulinum neurotoxin, commonly known as Botox. Botox is a neurotoxin that interferes with the formation of the SNARE complex, hinders acetylcholine release, and impairs muscle contraction. The result is a reduced appearance of wrinkles in the skin in the forehead, around the eyes, and above the upper lip. Stopping muscle contraction is even a useful tool outside of the beauty industry, as Botox can be used to treat muscle twitches, migraines, and hyperhidrosis.
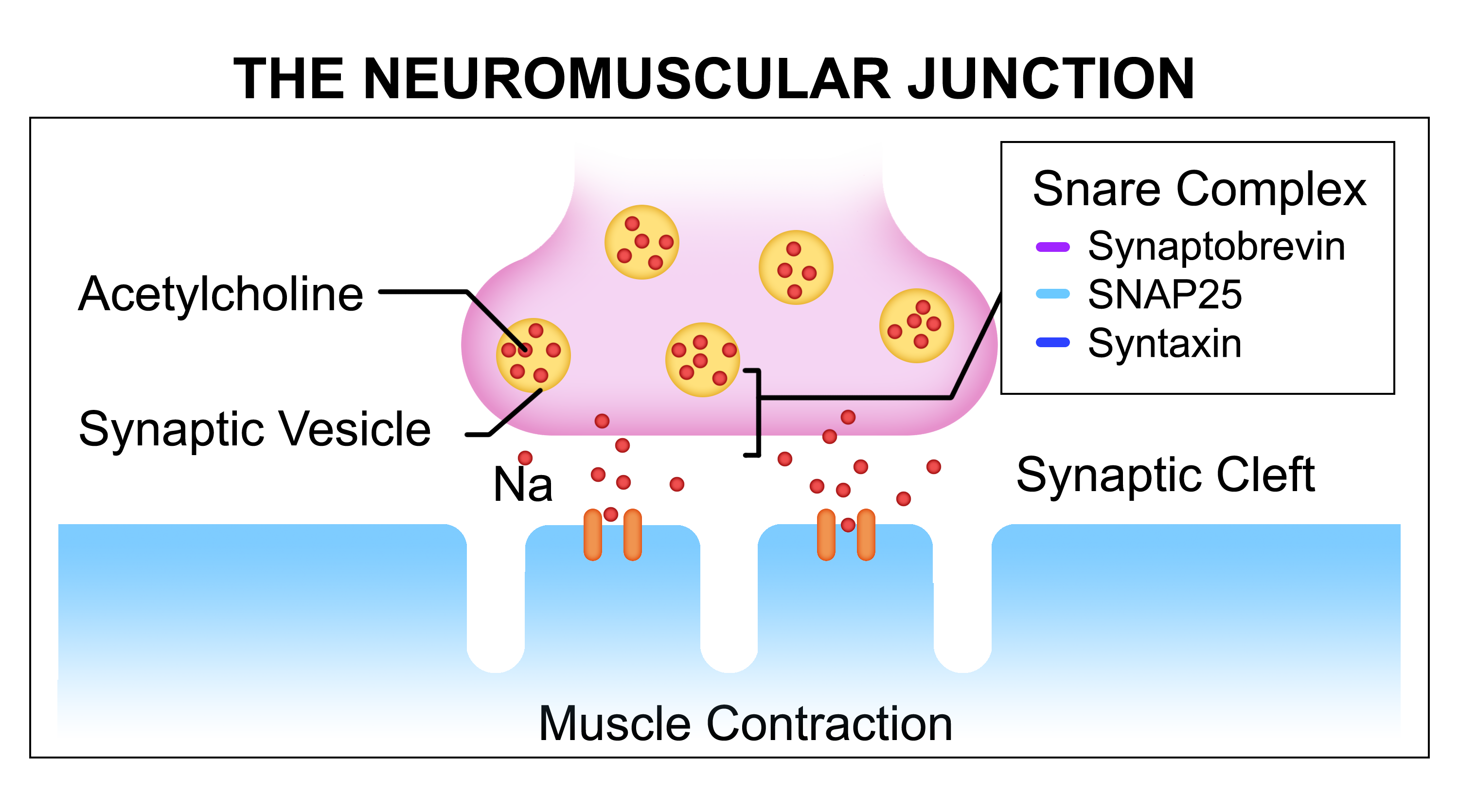
Acetylcholine from synaptic vesicles travels across the synaptic cleft, triggering a series of events that culminates in muscle contraction.
Botulinum toxin is a neurotoxin that prevents the formation of a functional SNARE complex. Different isotopes of this toxin target different SNARE proteins, but the end result is similar: inhibited ability to contract muscle fibers. Without a SNARE complex present, acetylcholine containing vesicles are prevented from fusing with the synaptic terminal membrane. Consequently, after Botox administration, there is no acetylcholine released from the neuron, and muscle contraction does not occur. Botulinum toxin was first isolated from a bacterium called Clostridium botulinum found on incorrectly preserved food, and has been FDA approved as a medication since 1989. Though it has existed as a medical treatment for quite some time, researchers at UC San Diego like Dr. Ruben Abagyan are still discovering novel ways to use botox as a therapeutic–namely, as a potential treatment for depression.
Dr. Abagyan’s research recalls the connection between muscle tension and mood that is bridged by the facial feedback hypothesis. This research builds on the notion that if muscles can no longer contract or remain tense as they do when the body is in depressive and stressful states, then perhaps the mind will also no longer receive signals that it should be depressed or stressed. Thus, Dr. Abagyan thought interrupting the facial feedback loop might help alleviate depression.
One way to stop such frown-associated facial contractions is through the use of Botox. Because Botox can inhibit muscle contraction, the injection of Botox into targeted facial locations can physically prevent individuals from frowning or wrinkling their forehead, both actions which manifest from tensed up muscles. This may work to reduce the negative effects of muscle tension, and may work to alleviate depressive emotions. On a more general level, Dr. Abagyan also thought that if facial muscles provide feedback that affects mood and emotions, it is possible that the contraction and tension of muscles throughout the body could also influence emotional states. Theoretically, a negative whole body state could contribute to a depression-enhancing feedback effect in the mind.
In his study, Dr. Abagyan injected Botox in patients who had been clinically diagnosed with depression. Across various patients, Botox was specifically administered into corrugator and procerus muscles (which produce the “angry wrinkle” on the forehead), upper and lower limbs, neck and eyelid muscles, or into the urinary bladder.
After six weeks, this placebo-controlled study showed that patients given a one-time Botox injection showed an improved score on the Hamilton Depression Rating Scale by an average of 47.1%, including patients who had taken prior depression medications with no satisfactory results. In contrast to these results, the placebo group showed only a 9.2% score improvement on average. Additionally, while current treatments for depression work differently for each patient and can take up to 4 to 6 weeks to become fully effective, reported antidepressant effects of Botox directly followed Botox administration. Results were self reported according to the Hamilton Depression Rating Scale, a 57-point scoring system that checks for symptoms of depression.
The specific location of the Botox injection was found to be somewhat insignificant: patients reported similar anti-depressant effects whether they received the injection in the face, limbs, or other areas of the body. This suggests that though Dr. Abagyan’s initial focus was to target facial muscles, preventing whole body muscle contractions produced similar antidepressant effects. Among the hypothesized explanations for these results is the facial feedback mechanism. It is possible that by reducing the amount of bodily tension from contracted muscles in the body and limbs, fewer signals that encourage negative thoughts are sent back to the brain. If this is indeed the mechanism by which depressive symptoms were alleviated, data may support Dr. Abagyan’s belief that disrupting the Facial Feedback Loop stops the circularity of negative thoughts and tensed muscles.
One criticism of this treatment is that instead of treating depression via the facial feedback hypothesis and associated body muscle tension pathways, Botox mitigates the condition by removing either cosmetic sources of depression or alleviating symptoms caused by chronic pain. In other words, instead of treating depression by disrupting the facial feedback loop, Dr. Abagyan may have simply alleviated feelings of negative self-worth associated with common signs of aging or symptoms of chronic pain that decrease quality of life.
The nature of the experiments involving Botox poses unique challenges for data evaluation and collection. For instance, blind studies are impossible to carry out as the administration of Botox can change a patient’s face drastically. So far, only firsthand accounts have been used to gauge efficacy. While this is not a foolproof method of determining effectiveness, accounts can be checked against statements given by other patients in control or placebo groups.
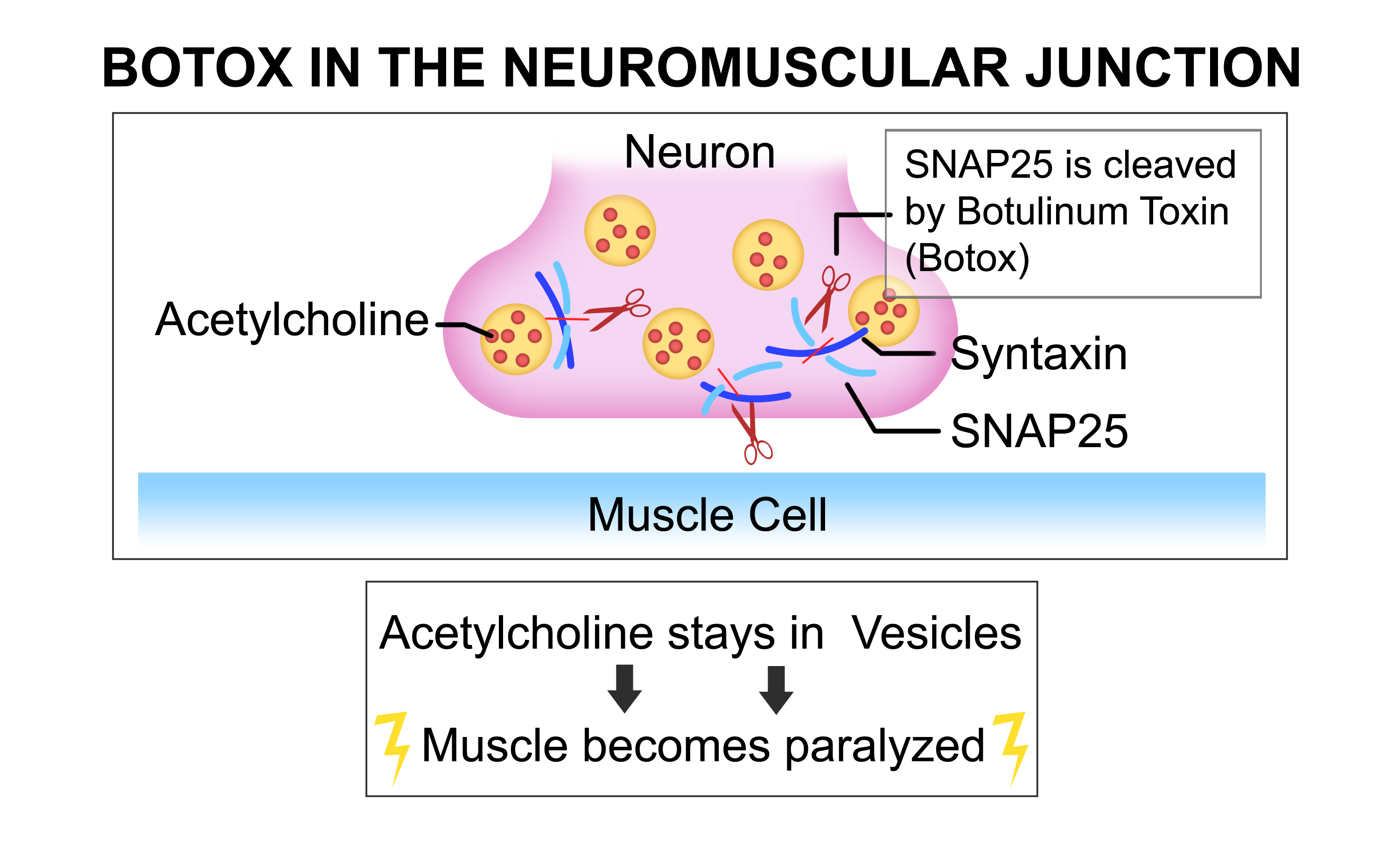
Botox inhibits the release of acetylcholine by disrupting the formation
of the SNARE complex. This ultimately impairs muscle contraction.
Depression is a major problem that afflicts many adults today. Because current treatments are often costly and require more than a month to reach full efficacy, it becomes increasingly important to research new avenues of antidepressant therapy. Current depression treatments have also been associated with a myriad of unwanted side effects, a development that can make the process of treating depression disheartening.â· This preliminary study carried out by Dr. Abagyan shows the potential of Botox as a relief for depressive symptoms, but further research will need to be conducted in order to demonstrate conclusively whether or not Botox can enter the field as a viable treatment for depression. Factors such as cost, side effects, and patient reluctance to administer Botox also need to be considered if any serious advancements are to take place.
Due to the preliminary nature of Dr. Abagyan’s studies and the prominent role patient self-reporting occupied in the experimental conclusions, the most we can say concerning Botox is that its administration is correlated with antidepressant effects. So far, however, Botox has shown a promising start as an unorthodox method of treatment as it seems to be at least somewhat helpful to some suffering with depression. Additional rigorous studies examining botox’s capacity to mitigate depression could lay the groundwork for an unconventional line of treatment for depression. Given the mounting stresses of daily life, it is now more important than ever to find antidepressant treatments that actually work.
Disclaimer: Dr. Ruben Abagyan is the co-founder of Molsoft, LLC, a drug discovery company, and owns equity.
REFERENCES
- Söderkvist, S., Ohlén, K., & Dimberg, U. How the Experience of Emotion is Modulated by Facial Feedback. Journal of Nonverbal Behavior 42, 129-151 (2018).
- Jacobsen, L. N. et al. Bodily symptoms in moderate and severe depression. Nord J Psychiatry 60, 294-298 (2006).
- Finzi, E., Rosenthal, N.E. Emotional proprioception: Treatment of depression with afferent facial feedback. Journal of Psychiatric Research (2016), doi: 10.1016/j.jpsychires.2016.06.009..
- Washbourne, P. et al. Genetic ablation of the t-SNARE SNAP-25 distinguishes mechanisms of neuroexocytosis. Nature Neuroscience 5, 19-26 (2002).
- Bhidayasiri, R., Truong, D. Expanding use of botulinum toxin. Journal of the Neurological Sciences 235, 1-9 (2005).
- Makunts, T., Wollmer, M.A., & Abagyan, R. Postmarking safety surveillance data reveals antidepressant effects of botulinum toxin across various indications and injection sites. Scientific Reports 10, 12851 (2020).
- Nalçakan, A.D. et al. Antidepressant awareness and stigmatizing attitudes toward depression and antidepressants, a comparison between first and sixth-year medical students. International Journal of Social Psychiatry (2021), doi: 10.1177/0020764020985545
WRITTEN BY SOHA KHALID
Soha is a Human Biology Major from John Muir College. She will be graduating in 2021.
FROM SALTMAN QUARTERLY VOL. 18
To read the original version, please click here. To read the full version on our website, please click here. To read more individual articles, please click here.