BY LAUREN BRUMAGE | UTS WRITER | SQ 2017-2018
[hr gap=”null”]
Prior to the advent of antibiotics, infectious diseases were the leading cause of death. In the era of modern medicine a silent killer pervades the human population. Cardiovascular diseases, which are responsible for 31% of deaths worldwide in 2012, have dethroned infectious disease as the leading cause of death (World Health Organization, 2016). Cardiovascular diseases are often considered diseases of affluence or mismatch illnesses arising from the modern lifestyle of plentiful caloric food to which humans are ill-adapted (Lieberman, 2013). However, cardiovascular diseases were also present in ancient times. In a study published in the International Journal of Paleopathology in March 2017, M. Binder and C.A. Roberts detail their research on the presence of heart disease in Amara West during the New Kingdom (1300 BCE to 1070 BCE) and Post-New Kingdom (1070 BCE to 800 BCE) periods. Their findings indicate that cardiovascular disease in the form of atherosclerosis impacted ancient humans of elite and non-elite backgrounds (Binder and Roberts, 2017). This indicates that cardiovascular diseases are not merely mismatch diseases arising from the contrast between the modern human lifestyle and the conditions of scarcity in which humanity evolved. Therefore, through examining the past via the bioarchaeological record, it is possible to further elucidate the causes and complexities of cardiovascular diseases.
The leading paradigm regarding cardiovascular diseases is that they are chiefly mismatch diseases. Humans evolved to be active and to store fat effectively for periods of scarcity, but the modern world is quite different from the landscapes in which humans evolved (Lieberman, 2013). Factors such as a diet high in fat and sugar, insufficient exercise, and hypertension are all byproducts of the modern lifestyle of relative plenty found in developed countries–and all of these factors are known to increase susceptibility to cardiovascular diseases (Binder and Roberts, 2017). From this perspective, cardiovascular diseases are clearly a result of a mismatch between the environment in which humans evolved and the contemporary cocoon humans have crafted. Yet there are other factors that are known to contribute to cardiovascular diseases that have nothing to do with mismatches. Infectious disease and genetic susceptibility to cardiovascular diseases are two such causative agents (Binder and Roberts, 2017). Although the perspective that cardiovascular diseases are mismatch illnesses certainly has some merit, it is an oversimplification of a complex collection of conditions.
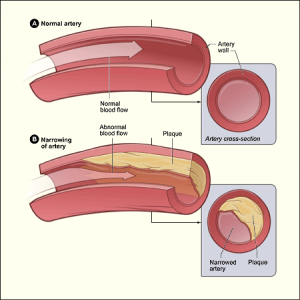
To further complicate the matter, the relative importance of each contributing factor to cardiovascular disease is not well characterized. There are also many clinical variants of cardiovascular disease, one of which is atherosclerosis. Atherosclerosis is the process through which arteries clog due to plaque buildup; over time, this accumulation of plaque can promulgate heart failure or arrhythmia (CDC, 2015).
Perhaps ironically, sometimes present ailments can be better understood through studying their presence in the past. Binder and Roberts led a team to the Ancient Egyptian provincial capital of Amara West (in modern-day Sudan) to study 180 corpses from the New Kingdom and Post-New Kingdom periods for signs of atherosclerosis. Thirty-six corpses came from the New Kingdom period and 144 came from the Post-New Kingdom period. Archaeological evidence indicated agrarian subsistence, and the prevalence of dental disease and trauma as observed with scanning electron microscopy indicated a difficult lifestyle (Binder and Roberts, 2017).

Of the 180 corpses, 5 had evidence of the arterial calcifications pathognomonic (characteristic) of atherosclerosis. Due to differential preservation of calcifications and difficulty in recovering calcified structures intact, it is possible that more individuals buried at Amara West had calcifications. According to Binder and Roberts, arterial calcifications have been found in other ancient samples–in mummies from Egypt, Peru, China, and the Arctic. However, most of those mummies had an elite or even royal background so in life the individuals would have had greater access to resources such as richly caloric food and high-quality shelter. Therefore, these individuals may have led more “modern” lifestyles in terms of food consumption, indicating cardiovascular disease as a mismatch disease or as a disease of affluence. The Amara West finds presented in this study are significant in that that 4 of the 5 corpses showing signs of atherosclerosis are from non-elite contexts (Binder and Roberts, 2017). These individuals did not lead lives of leisure; rather, they were agriculturalists who made their living through strenuous labor.

If 4 of the corpses with atherosclerosis come from more humble backgrounds, what may have caused the pathology? In this case cardiovascular disease is clearly not present as a mismatch illness or a disease of affluence. All of the corpses with evidence of atherosclerosis also have indicators of chronic respiratory disease. The authors cite recent research indicating that bacterial pneumonia can facilitate the development of cardiovascular disease, so it is possible that this was the cause of atherosclerosis. Furthermore, in modern populations tobacco smoke is linked to respiratory pathologies as well as to atherosclerosis. Binder and Roberts suggest that consistent exposure to smoke from cooking fires may produce a similar effect, noting that archaeological data from the Amara West ruins indicate consistent use of hearths and ovens without sufficient ventilation (Binder and Roberts, 2017).
It is clear from modern clinical work and from the research of Binder and Roberts at Amara West that cardiovascular diseases have a multiplicity of causes that are often difficult to evaluate. Cardiovascular diseases are clearly not just modern mismatch illnesses since they manifested in ancient populations among individuals who lived in conditions of scarcity. In fact, the findings of Binder and Roberts point to infectious diseases of the respiratory system and to exposure to smoke as potentially important causative factors in atherosclerosis. Further research into the various causes of cardiovascular diseases will allow clinicians to more readily identify at-risk patients and prescribe more effective precautionary measures. While it is imperative to conduct additional research into the pathology of heart disease in living populations, the bioarchaeological record should not be neglected as it has the potential to provide a wealth of information. Genetic causes of cardiovascular diseases were not explored by Binder and Roberts, but it would be possible to combine the osteological analysis present in this study with ancient DNA technology to investigate this in the bioarchaeological record. By examining the health of past populations, it is possible to gain additional insight into the causes of diseases that endure in the present day.
References
Amara West, West gate [Photograph]. Retrieved from http://www.bsr.ac.uk/research/archaeology/geophysics-2/projects/amara-west-sudan
Atherosclerosis [Diagram]. Retrieved from https://www.nhlbi.nih.gov/health/health-topics/topics/atherosclerosis
Binder, M. and Roberts, C.A. (2017). Calcified structures associated with human skeletal remains: Possible atherosclerosis affecting the population buried at Amara West, Sudan (1300-800 BC). International Journal of Paleopathology, 6(2014) 20-29.
(2016). Cardiovascular diseases (CVDs). Retrieved from http://www.who.int/mediacentre/factsheets/fs317/en/
(2015). Coronary Artery Disease (CAD). Retrieved from https://www.cdc.gov/heartdisease/coronary_ad.htm
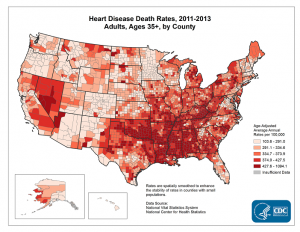
Heart Disease Death Rates, 2011-2013 Adults, Ages 35+, by County [Computer-generated map]. Retrieved from https://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_heart_disease.htm
Hill, Joseph. (2016). Why it’s time to care about the heart disease epidemic. Retrieved from http://www.utswmedicine.org/stories/articles/year-2016/heart-month.html
Lieberman, D. (2013). “Survival of the Fitter: Can Evolutionary Logic Help Cultivate a Better Future for the Human Body?” In The Story of the Human Body: Evolution, Health, and Disease (368-388). Knopf Doubleday Publishing Group. Web.
Localization of Atherosclerosis [Graphic]. Retrieved from http://www.bloodflowonline.com/perspectives/localization-atherosclerosis.